
Medical Marijuana?

NY Physicians Reluctant To Prescribe Medical Marijuana As Alternative To Opioids For Chronic Pain.
Crain’s New York Business (1/29, Lewis) reports that although medical marijuana “offers an alternative to opioid drugs for treating chronic pain,” most physicians in New York “are still reluctant to embrace cannabis as a medical treatment.” According to Crain’s, “only 833 physicians, about 1% of the state’s total, are certified to prescribe the drug.” The article mentions that the Medical Society of the State of New York wrote a letter to the state Health Department in December that “called the plan to approve cannabis for treating chronic pain premature.
At His Branches Health Services we agree with the Medical Society of the State of New York for a number of reasons. “Marijuana” is a plant, not a medication, that has many psychoactive phytochemicals in it with varying actions, properties, and strengths. Some may have a beneficial effect on relieving pain but others alter consciousness and expose patients to mental health risks as well as impairing their ability to drive carefully and handle dangerous machinery. Before the active ingredient in marijuana that is beneficial in pain relief has been clearly isolated, carefully studied, and is available in a pure form with reliable dosing and instructions, its use should remain seriously limited.
Population Health

What does the future hold?
In a series of article on Population Health this week in Medical Economics (click on image below) the authors discuss a number of recent developments in medical practice that we’ve been actively involved in at His Branches Health Services over the past few years. One of the primary questions is, how will these changes be affected by the recent shift in power in Washington, DC?
What is “population health”? By definition it is “the health outcomes of a group of individuals, including the distribution of such outcomes within the group,” and in a primary medical care practice like ours it is an organized approach to health care that aims to improve the health not only of individual patients but of all of the patients in our clinic practice and surrounding community.
The excerpt below (click here for full article) suggests that the future of population health is well-established and here to stay.
David Nash, MD, MBA, and dean of Jefferson College of Population Health at Thomas Jefferson University in Philadelphia, Pennsylvania, told Medical Economics that the Affordable Care Act (ACA) has shifted the healthcare cost structure, increased the demand for greater accountability and requires primary care physicians to focus on groups of chronically ill patients that cost more to the healthcare system.
“The horse is so far out of the barn you can’t see its tail,” Nash said. “The most important issue in healthcare is how we reduce costs in the system, and the move to value-based care is inexorable.”

High Prices for Drugs With Generic Alternatives

The Curious Case of Duexis
Aaron Hakim, MS and Joseph S. Ross, MD, MHS
JAMA Intern Med. Published online January 23, 2017. doi:10.1001/jamainternmed.2016.8423
Approximately 13% of health care expenditures in the United States are for prescription drug spending, nearly $420 billion in 2015. High-priced pharmaceuticals, therapies that cost more than $600 per month, are projected to eclipse 50% of total drug spending by 2018. Price increases for these therapies have been persistent, with unit costs increasing 164% between 2008 and 2015. Pharmacy benefit managers are third-party administrators that process and pay prescription drug claims and negotiate drug prices with manufacturers.
Pharmacy benefit managers have sought to manage prescription drug use and mitigate cost increases through such measures as prior authorization and step therapy requirements for physicians, increased copayment requirements for patients, and exclusion of some expensive medications from health plan formularies. Using the illustrative example of Duexis, a single-tablet, fixed-dose combination of the nonsteroidal anti-inflammatory (NSAID) ibuprofen [Advil] and the histamine H2-receptor antagonist famotidine [Pepcid] marketed by Horizon Pharma (Dublin, Ireland), we describe how some pharmaceutical companies have sought to circumvent such restrictions and maintain high prices for drugs, even for those with generic alternatives.
Duexis was approved by the US Food and Drug Administration (FDA) in 2011 to relieve symptoms of osteoarthritis and rheumatoid arthritis and to decrease the risk of developing gastric and duodenal ulcers in patients at risk for NSAID-associated ulcers. After approval, Duexis was first marketed at an average wholesale price, a benchmark used for pricing and reimbursement of prescription drugs, of $158.40 per month.
The drug is a combination of 2 over-the-counter medications that are sold as generics and would cost approximately $16 per month if purchased separately at the same doses. Since 2012, Duexis has had 11 price increases (see Figure below). As of August 12, 2016, the monthly wholesale price was $2061, representing a 1131% aggregate increase. In 2015, nearly $200 million was spent on Duexis in the US, with estimated cumulative revenue over 5 years of more than $600 million since FDA approval.
Figure
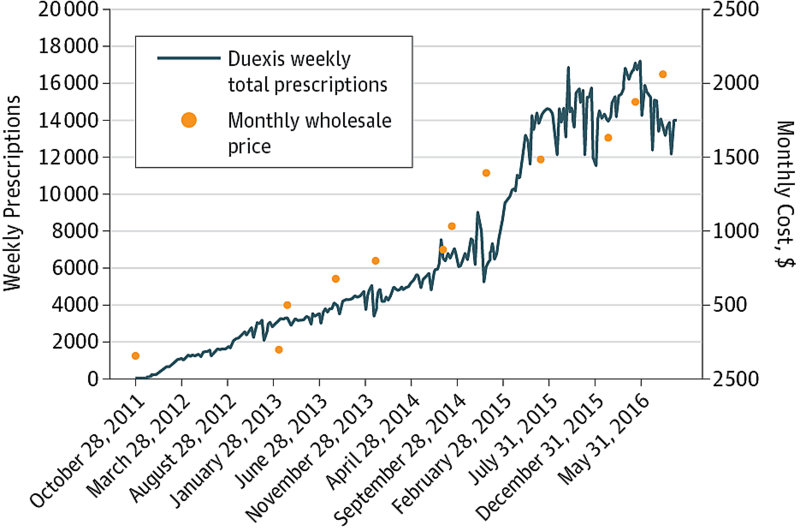
Weekly Prescriptions for Duexis and Monthly Wholesale Price After Each of the 11 Price Increases Since October 2011, When Duexis Was First Made Available in the United States
Pharmaceutical companies employ several tactics to offset prior authorization, step therapy, and other utilization controls imposed by pharmacy benefit managers on physicians. Horizon, for example, has physicians submit Duexis prescriptions directly to an affiliated mail-order specialty pharmacy, which prepares the prior authorization paperwork and provides medical justification to the pharmacy benefit manager on behalf of the physician, reducing the administrative burden. Horizon reports that 70% of Duexis prescriptions are filled through their “Prescriptions Made Easy” specialty pharmacy program. One such specialty pharmacy, Linden Care, has 59% of its business dedicated to dispensing drugs made by Horizon Pharma. In 2016, the US Attorney’s Office for the Southern District of New York was investigating Horizon’s specialty pharmacy practices.
Click here to read the full article in the Journal of the American Medical Association (JAMA).
HPV high in men
The first national estimate
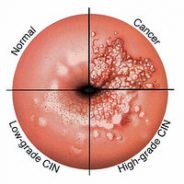
suggests that nearly half of US men have genital infections caused by a sexually transmitted virus and that one in four has strains linked with several cancers, the Associated Press reports. Most human papillomavirus infections cause no symptoms and disappear without treatment, and most adults will get an HPV infection at some point in their lives. But high-risk HPV can cause cancer in the mouth and upper throat, cervical cancer in women, and other cancers; less harmful strains can cause genital warts.
Who is at risk?
Vaccines can prevent infections, but experts say vaccination rates in pre-teens and young adults are too low. High-risk HPV poses cancer risks to people who are infected and to their sexual partners, who can catch HPV even when the infections are silent.
The findings come from an analysis of a 2013-14 national health survey; nearly 2,000 men ages 18 to 59 were tested for HPV, with results published Thursday in the journal JAMA Oncology. Researchers say it’s the first published estimate for genital HPV infections in men. The 45% rate is higher than previously reported rates for women, per lead author Dr. Jasmine Han.
HPV is the leading cause of cervical cancer, but HPV-related mouth and throat cancers are becoming more common, especially among men, who aren’t routinely screened for the virus.
Behavioral change and vaccination indicated
A University of Chicago head and neck cancer specialist says the results show doctors and parents need to step up efforts to vaccinate boys and young men and get over concerns that the HPV vaccine will lead to risky sexual behavior.

Vaccine Controversy?

Benefits are a matter of fact
I have started, scratched out and even abandoned the writing of this essay. I couldn’t do it. It wasn’t there. Didn’t feel it.
Something kept nagging at me, and it took some time to finally figure out what it was. It’s the idea that this article would be labeled “opinion” or “editorial” in the first place.
Sure, there are some topics that seem to lend themselves appropriately to opinion pages. Vaccines, however, which have prevented 6 million deaths every ear worldwide and have fundamentally changed modern medicine, should not be on that list.
The benefit of vaccines is not a matter of opinion. It is a matter of fact.

Studies, including a meta-analysis of 1.2 million children in 2014, show no link between vaccines and autism. That is not a matter of opinion. It is a matter of fact.
That you are 100 times more likely to be struck by lightning than to have a serious allergic reaction to the vaccine that protects you against measles is not a matter of opinion. That is also a matter of fact.
Facts should matter, and science should win, but after 13 years as a medical reporter, I know it is not that simple.
Science often loses the zeal argument to ideology, and in some ways, it is easy to understand why.
At the heart of the vaccine argument is the awesome challenge of trying to prove a negative.

If you or your child never gets the disease the vaccine was designed to prevent, there is no surprise. There is no headline. Life goes on.
The flip side, though, is the one-in-a-million child (literally, 1/1,000,000) who has a serious adverse reaction. It is likely to make the news, confirm the worst fears and lead to the enlistment of an army in the fight against vaccines.
Click here to read the entire CNN article by Dr. Gupta.
Teen Virginity Beneficial
The sexual choices and values our young people hold have real-life consequences far beyond sexuality itself.
In my nearly 25-year career at Focus on the Family as a social science researcher, I am constantly amazed and encouraged in my faith at how what God requires of us in our familial and sexual lives is never contrary to good, honest science. The two correspond in remarkable ways. And why shouldn’t it? When sociologists study the behaviors of man without agenda, they unwittingly discover the rightness of God’s wisdom and care in His directions to us. The scholars just don’t realize it. We as believers should.
This is demonstrated in a new report from the United States Centers for Disease Control (CDC). It’s the first ever of its kind, examining a very large and diverse array of health behaviors of high school students according to their self-reported sexual activity. What makes this report particularly interesting, beyond its categorization by sexual activity, is it examines widely varied safety and health behaviors from bike helmet and seat belt use to substance abuse, diet, doctor’s visits, exercise and even tanning bed use. The two major conclusions from the report are quite stark:
- The virginal students rate significantly and consistently better in nearly all health-related behaviors than their sexually active peers. They do so by remarkably stunning measures.
- Teens who have sexual contact with the same or both sexes have remarkably lower percentages of healthy behaviors overall than their heterosexually active peers.
An additional report conducted by Child Trends, a Washington, DC-based think tank focused on children’s health, adds to the robust research literature on this topic. It finds that teens from homes where mother and father have a healthy relationship, both have warm, monitoring relationships with their children and the family has regular, dependable schedules and practices at home are substantially less likely to be sexually active by every measure.
Here’s a sampling of various measures the CDC examined and the health disparities between the three categories of students: virginal, heterosexual and same-sex or bi-sex sexually active.
- Seat Belt Use: Opposite-sex-active (OSA) teens are 143% more likely to never or rarely wear a seat belt than their virginal peers. Same-sex/bisexual active (SS/BA) teens are 317% more likely than their virginal peers.
- Passenger w/Drinking Driver: OSA teens are 94% more likely to ride with a driver who’s been drinking than their virginal peers. SS/BA teens are 115% more likely than virginal students.
- Dating Violence: OSA teens are 260% more likely to experience some form of physical violence in dating relationships than virginal peers. SS/BA teens are 683% more likely than virginal youth.
- Smokes Daily: OSA teens are 3300% more likely to smoke daily than virginal peers. SS/BA teens are 9500% (you read that right) more likely than their virginal classmates.
- Ever Binge Drank: OSA teens are 337% more likely to ever binge drink than virginal peers. SS/BA teens are 375% more likely than virginal their peers.
- Pot Use: OSA teens are 336% more likely to be currently using marijuana than their virginal peers. SS/BA teens are 483% more likely than the virginal.
- Ever Injected Illegal Drug: OSA teens are 500% more likely to have ever injected a non-prescription drug than virginal peers. SS/BA teens are 2333% more likely.
- Felt Sad of Helpless: OSA teens are 48% more likely to report feeling so sad or helpless almost every day for 2 or more weeks in a row that they stopped doing some of their usual activities compared to their virginal peers. SS/BA teens are 181% more likely to feel this way compared to virgins.
- Tanning Beds: OSA teens are 282% more likely to use indoor tanning beds than their virginal peers. SS/BA teens are 364% more likely than virginal peers.
- Eat Breakfast Daily: OSA teens are 24% less likely to eat breakfast daily than virginal peers. SS/BA teens are 48% less likely than virginal classmates.
- Eight Hours Sleep: OSA teens are 21% less likely to get 8 hours of sleep a night than virginal peers. SS/BA teens are 34% less likely than virgins.
- Asthma: OSA teens are 24% more likely to have ever had asthma than virginal peers. SS/BA teens are 48% more likely.
- Physical Fight: OSA teens are 133% more likely to have been in a physical fight than virginal peers. SS/BA teens are 187% more likely.
- Dentist Visit: OSA teens are 8% less likely to have visited the dentist in the last year than virginal peers. SS/BA teens, 20% less likely.
It is intriguing to note how many of these health measures have no seemingly direct relation to sexual activity and decision making itself, even tangentially; things like seat belt use, eating breakfast daily, smoking, dentist visits, illegal drug use, suffering from asthma, etc. Obviously, there’s a curious and meaningful relationship between our teens’ sexual values/activity and a substantial number of unanticipated but very consequential health behaviors.
What is more, this data seems to challenge the popularly held charge that same-sex and bi-sexual sexually active kids have these more troubling measures and higher risk of attempted suicide because their sexuality is not affirmed by the larger society. This is used as accusation against those of us who cannot support any non-marital sexual behavior. We are told that people like us are responsible for such tragic outcomes. It’s no minor charge. But is it true?
If it were, it would follow that opposite-sex sexually active kids are taunted and rejected for their sexuality as well given their remarkably high levels of unhealthy behaviors and higher levels of suicidality than the virginal. This, of course, it would also mean that the virginal are the most widely accepted, celebrated and encouraged students at school. Does anyone believe that?
This “accept-our-sexuality-or-we-die” accusation also faces stiff challenge by the fact that even in the most gay-affirming countries in the world, these imbalances in health measures and suicidality are present. In fact, there is nowhere in the world where the hetero and homosexual measures, in general are close. That is seen in research of same-sex identified adults in places like Scandinavia, the Netherlands and Switzerland. See here, here, and here for example.

It’s difficult to determine from this CDC report alone just how these various measures are related to one another. Does sexual activity drive the increase in other negative health behaviors, vice versa or if at all? This data does not say. But the fact that the CDC measured all these health behaviors by sexual activity and distributed it to health professionals around the world in this major report certainly indicates their relationship is of significant interest to health-care workers.
These findings should be very concerning to all parents and professionals concerned with our teens’ general health and well-being. The sexual choices and values our young people hold have real-life consequences far beyond sexuality itself. Thus, there are indeed compelling reasons to encourage teens to choose not to be sexually engaged with peers of the opposite or same-sex.
Our children should know there’s very compelling scientific evidence on so many levels showing how saving the precious gift of their sexuality for the safe harbor of marriage is not about old-time moralism or unhealthy sexual repression. Just the opposite is true. Chastity is related to so many substantial measures of human health and well-being that it should be strongly appreciated by parents, health and education professionals as one of the most important health boosting factors for our nation’s young adults.
 by Glenn Stanton
by Glenn Stanton
Glenn T. Stanton debates and lectures extensively on the issues of gender, sexuality, marriage and parenting at universities and churches around the world. He is the author of eight books on families, theology and gender and contributor to many others. His latest two are Loving My (LGBT) Neighbor: Being Friends in Grace and Truth and The Ring Makes All the Difference.
“Mommy brain”

Pregnancy may change mom’s brain for years afterward
According to an article in this week’s STAT News, neuroscientist Elseline Hoekzema and colleagues have studied brain plasticity — that is, the way the adult brain changes — for years. But it wasn’t until one of her colleagues was trying to become pregnant that the team started pondering questions of how pregnancy and motherhood change a woman’s brain.

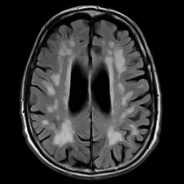
What they found was that pregnancy reshapes the brain for at least two years afterward, with strongest effects in regions of the brain that are involved in social processing and those that respond to their child’s face. Those changes, the scientists say, may prepare a woman for the social demands of motherhood.
Previous animal studies have established that reproduction leads to long-lasting changes in brain and behavior. And scientists have long understood that hormones can change brain structure and function.
But there have been few human studies. A widely reported nine-cohort study from 2002 helped create the popular idea of memory difficulties (or “momnesia”) and a general “fuzziness” in thinking as a result of having been pregnant.
Hoekzema and colleagues at the Autonomous University of Barcelona wanted to investigate how the brain physically changed in mothers. They recruited 25 first-time mothers and performed MRI brain scans both before conception and after birth, looking for pregnancy-induced structural changes in the women’s brains’ gray matter.
Their brains were compared to the brains of 19 first-time fathers (scanned both before and after their partner’s pregnancy), 17 men without children, and 20 women who had never given birth.
The scientists observed that first-time mothers, but not fathers, exhibited reduced gray matter in brain regions associated with the ability to attribute thoughts, feelings, and intents to themselves or other people. But that doesn’t mean that those social capabilities were dampened — on the contrary, the researchers think the shrinkage was evidence of maturation of those social networks. Other studies have shown that pregnant women have enhanced emotion and face recognition.
Mothers with the greatest gray matter shrinkage had the highest quality of mother-to-infant attachment after birth. And a follow up imaging session found that almost all of these brain changes lasted for nearly two years after giving birth. The study was published Monday in Nature Neuroscience.
Hoekzema and her colleagues are now working on follow up studies based on their findings. Specifically, they want to examine how the regions of reduced brain volume are working together in the new mothers, and find out if the brain changes can predict the emergence of postpartum depression. They also want to find what happens to women’s brains after multiple pregnancies.
“This has opened up a complete new line of investigation, and I imagine we will be studying this for many years to come,” Hoekzema said.
Statins and Alzheimer’s
Regular Use Of Statins May Be Associated With Reduced Risk For Alzheimer’s, Study Suggests.
ABC World News Tonight (12/12, Story 10, 0:20, Muir) reported, “A new study shows that high use of cholesterol lowering statins is now tied to a lower risk of Alzheimer’s for patients over the age of 65.”
CNN (12/12, Howard) reports that research published online Dec. 12 in JAMA Neurology suggests “regular use of statins is associated with a reduced risk for Alzheimer’s.” The research “involved Medicare data on 399,979 statin users.” Investigators “found that those who were exposed to higher levels of statins… were 10% less likely to have an Alzheimer’s disease diagnosis in each of the subsequent five years than those with lower statin exposure.”
HealthDay (12/12) reports that researchers found, however, that “it may depend on the specific statin, and the gender and race or ethnicity of the person taking it.” For instance, “black men appeared to gain no benefit from taking any statin, while white women may lower their risk regardless of which statin they take, the researchers said.”
Overdose deaths rising
Opioid-Related Deaths at All-Time High
The Washington Post (12/8, Ingraham) reports data released by the Centers for Disease Control and Prevention on Thursday revealed that “opioid deaths continued to surge in 2015, surpassing 30,000 for the first time in recent history.”
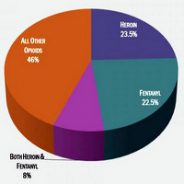
The data shows “an increase of nearly 5,000 deaths from 2014.” CDC Director Tom Frieden said in a statement, “The epidemic of deaths involving opioids continues to worsen.” He added, “Prescription opioid misuse and use of heroin and illicitly manufactured fentanyl are intertwined and deeply troubling problems.”
The AP (12/8, Stobbe) reports that according to the data, overdose deaths rose “11 percent last year, to 52,404.” The AP specifies that “heroin deaths rose 23 percent in one year,” deaths “from synthetic opioids, including illicit fentanyl, rose 73 percent,” and abuse “of drugs like OxyContin and Vicodin” increased 4 percent.
Robert Anderson, “who oversees death statistics at the Centers for Disease Control and Prevention,” said, “I don’t think we’ve ever seen anything like this. Certainly not in modern times.” The amount of deaths from overdose was greater than that of car crashes and gun violence.
CNN (12/8, Almasy) also covers the story.
Who is Tom Price?

10 Things to know
about HHS Secretary designate Tom Price
By Medical Economics staff, November 29, 2016
Tom Price, MD, a Republican representative from Georgia, is poised to be nominated as the next secretary of the U.S. Department of Health and Human Services, according to media reports. Here’s what physicians should know about Price.
10. He is a third generation physician, having served in private practice for nearly 20 years in Georgia as an orthopedic surgeon. He received his bachelor’s and medical degrees from the University of Michigan and completed his orthopedic surgery residency at Emory University in Atlanta. Price later returned to Emory as an assistant professor and medical director of the orthopedic clinic at Atlanta’s Grady Memorial Hospital, where he taught resident physicians.
9. Price is a member of the GOP Doctors Caucus. The caucus is comprised of 18 medical professionals who use their medical training and expertise to help shape healthcare policy.
8. Price is a six term member of the house, first elected to represent Georgia’s 6th district in 2004. He serves on the House Committee on Ways and Means and is chairman of the House Budget Committee.
7. He is a vocal critic of the Affordable Care Act. In October, Price blasted the Obama Administration following news of premium rate hikes on some marketplace based health plans in a statement: “…President Obama and Democrats have the audacity to tout Obamacare’s ‘success,’ [but] the cold hard facts and figures prove the opposite is true.” A few days earlier, he pledged that Republicans would fight for “patient centered solutions that actually put patients, families and doctors in charge of healthcare in this nation.”
6. Price is a key proponent of House Speaker Paul Ryan’s (R Wisconsin) “Better Way” plan to repeal and replace the Affordable Care Act. As one of the House Republicans who devised the plan, Price recently said it was “simply not enough” to acknowledge the failures of Obamacare, but it’s necessary to offer another solution.
5. He is not completely sold on the final rule for the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA), although he voted for the legislation. Following the release of the final rule in October, Price said Medicare’s new Quality Payment Program “deserves careful scrutiny in the light of serious concerns” among the GOP Doctor’s Caucus. “We are deeply concerned about how this rule could affect the patient-doctor relationship, and I look forward to carefully reviewing it in the coming days to determine whether the Administration has addressed those concerns and put the interests of patients first” Price said via statement.
4. Price is a Trump supporter. In May, as chairman of the House Budget Committee, Price joined eight fellow chairmen in endorsing Trump for president. “Any other outcome [of the election] is a danger to economic growth, puts our national security in peril, enshrines ObamaCare as the law of the land, entraps Americans in a cycle of poverty and dependence, and undermines our constitutional republic,” Price and his colleagues wrote.
3. Price and fellow Republicans have their eye on Medicare reform as an immediate priority. Earlier this month, Price told reporters that reforms to the federal program would likely come “six to eight months” into a new administration. Media reports say both Price and Speaker Ryan support privatizing Medicare, but no specific plans have been unveiled.
2. Price supports Medicaid reform as well, recently calling the program “an empty promise” in the 2017 House budget committee’s resolution. Price added, “Finding a physician who will see Medicaid beneficiaries can be incredibly challenging because providers are under-reimbursed and cannot afford to provide care at the rates the program pays.”
1. Price is very active on Twitter. Find him @RepTomPrice.
Meet Our CEO, Dr. Morehouse
 I'm a happy person who loves getting to know and being able to help people of all ages. I connect with little children (and the little child in most adults) almost immediately. Sharing the joys and trials of relationships, pregnancy and delivery, and family life are the things about family practice that really light my fire. I've found that having a sense of humor and seeing God's love at work can see us through some of life's most difficult times, if we can keep the faith and hang in there together.
I'm a happy person who loves getting to know and being able to help people of all ages. I connect with little children (and the little child in most adults) almost immediately. Sharing the joys and trials of relationships, pregnancy and delivery, and family life are the things about family practice that really light my fire. I've found that having a sense of humor and seeing God's love at work can see us through some of life's most difficult times, if we can keep the faith and hang in there together. 


